| Hyperhidrosis USA - Micro ETS | Call 210-490-7464 Email info@dhnmd.com | The Offices of David H. Nielson, MD | |
 |
|
 |
 |
![]()
![]()
![]()
Repeat ETS Surgery for Recurrent Sweating SymptomsIntroduction Partial nerve regeneration has also been found in many redo surgeriesby Dr. Nielson on patients who had a sympathectomy by another doctor. Much less commonly, persistent symptoms is due to mis-identifying the T3 as the T2 level and therefore leaving the T2 level completely untouched and free to carry sympathetic nerve signal to the fingers and face.
December
2012 Successful
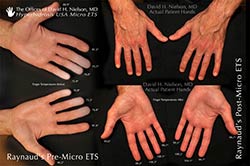
Redo ETS R2 caused warming of cold 3/4/5 fingers of both hands!
April 2008 CT guided Thermal (RFA) Sympathectomy of T2. Redo surgery of patient who was not a candidate for traditional ETS due to adhesions of the left lung covering the 2nd and 3rd rib heads. (Click to See) April 2008 Only the second patient to have CT guided Thermal (RFA) Sympathectomy of T2. Redo surgery of patient who was not a candidate for traditional ETS. (Click to See) Previous surgeries by another doctor unsuccessful, Dr. Nielson performs successful repeat surgery:
Why have people come to you to have redo Micro ETS surgery?
T2 Sympathetic Innervation to The Sweat Glands of the Face Over several years of experience in treating patients with recurrent and/or persistent sweating of the face after undergoing T2 sympathectomy, I have found that persistence of any sympathetic nerve innervation across the second rib level, just above the T2 ganglion, plays a significant role in persistent sweating conditions of the face after undergoing a T2. T3, or T4 sympathectomy. It is apparent in some patients that there are neuronal contributions from lower levels such as the T3 that pass up over the second rib level on their way to the face that participate in the sweating symptoms of the face. Some physicians misunderstand the sympathetic nerve innervation of the face and believe in order to treat facial sweating it is important to cut the sympathetic nerve at the T1 level or above, thereby causing the dreaded Horner’s Syndrome. This, in my experience, I’ve found not to be the case. In summary, for successful treatment of facial sweating, it is imperative that all sympathetic nerve innervation crossing the second rib level be divided as opposed to clamped or having lower levels cut or clamped. Also, accessory nerve branch pathways bypassing the T2 ganglion can or may contribute to persistent facial symptoms. Case Histories and Results
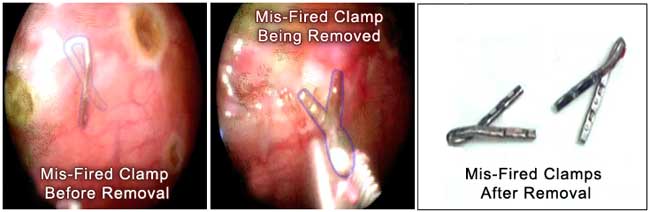
Patient had persistent facial sweating after clamping/cutting of the T2. Dr. Nielson did a redo on him and found that the clamps had fallen off the nerve where they had been placed just above the T2 ganglion on both sides. Dr. Nielson reduced patient's facial sweating (forehead) by cutting the nerve at the 2nd rib level. His previous surgeon had told him that his persistent forehead sweating after T2 clamping/cutting was due to T1 innervation to his eye which if cut to reduce his forehead sweating would also cause Horner's syndrome. This wasn't the case and Dr. Nielson successfully treated his persistent forehead sweating by precisely cutting the sympathetic nerve at the upper border of the 2nd rib.
Patient had two previous surgeries with clamps
at 2nd, 3rd, and 4th ribs. His facial blushing was not resolved
with either surgery, he developed severe CS and facial sweating.
Twelve days after surgery patient reports facial blushing seems
to be getting a little bit better everyday. Rates his facial blushing
as a 1 (on a scale of 1 to 3, being the most severe), but says
he hasn't really been in a situation that would trigger the most
severe episode of facial blushing.
Professional prior to first ETS was terrible. After has been great, however recurring symptoms are beginning to effect again. Social and personal have been better since first ETS as a whole. Since nearly every social activity involves eating, however, the gustatory sweating has made life miserable from that standpoint. The Levsin takes an hour to kick in and you can't do anything spontaneously that way. Gustatory sweating began 6 mo post op, hands are still warm and dry after first ETS, all other symptoms started about 4 years post op (facial blushing and sweating). CS of the chest is moderate, worse with heat and humidity. Patient thinks the surgeon cauterized T2 bilaterally. Gustatory sweating started one month after surgery. 3/20/98 Patient has bilateral T2 in Sweden. Bilateral cautery distruction of the T2 ganglia. Palmar sweating ceased. 6 months later gustatory sweating developed. 4 years after surgery, severe Blushing and moderate facial sweating and moderate cold hands (but hands still dry) developed. 8/20/03 Dr. Nielson performs micro ETS of T2(above) (5 years after patient had undergone ETS) and Blushing resolved along with facial sweating.
22 year old white male underwent ETS-C (clamping) of T2 for severe Blushing and mild palmar hyperhidrosis. Four months later he presented with persistent severe cranio-facial erythema (blushing) and mild hyperhidrosis of the palms despite ETS-C of T2. Micro ETS of T2(above) was then performed (by me) with precise division of the sympathetic nerve at the 2nd rib bilaterally. The titanium clamp was across the nerve 4 mm below the 2nd rib on the right and had become dislodged from the nerve and was lying 5 mm away from the nerve on the left side. Complete resolution of Blushing and palmar hyperhidrosis occurred after bilateral Micro ETS of T2(above).
29 year old asian male with severe Blushing, facial sweating and mild palmar sweating who underwent ETS-clamping of T3/T4 without improvement in his facial symptoms and developed cs (compensatory sweating). His hands had become mostly dry but were still slightly cool. One month later he elected to have ETS-clamping of T2 without any improvement in his facial blushing or sweating and no change in his cs. He then presented to me 20 months later to haveMicro ETS of T2 (above) with division (cutting) of the nerve where it crossed the 2nd rib. Dense lung adhesions to the 2nd and 3rd rib heads made it too invasive to remove the clamps. The nerve was divided where it crossed the 2nd rib head using the tips of micro endoshears. Immediate significant decrease in both Blushing and facial Hyperpyrexia (burning) symptoms occurred as well as facial sweating. His fingers became warm too. No change in the degree of cs that he had preoperatively.
Persistent
facial blushing after sympathectomy can occur if any kuntz nerve
that crosses the second thoracic rib is left intact, and can
therefore continue to carry nerve signals to the face. Kuntz nerves that arise from T4 can actually cross the second rib several inches lateral to the main sympathetic nerve trunk, making them easily missed especially if not examined from an optimized angle and if the surgeon's technique is one where only very large Kuntz nerves can be seen. In instances such as these, the incidence of finding Kuntz nerves is reportedly as low as 5 to 20%.
Re-do patients tell us their post op pain and recovery is much less with re-do than their original surgery.
A 24 year old white male sufferred from severe blushing with severe facial hyperpyrexia (face/head heat) and moderate palmar hyperhidrosis for 14 years. These symptoms were refractory to Ativan, Valium, Effexor and Prozac. He elected to undergo bilateral ETS of T2 by clamping technique three months ago. At that time, two clamps were placed above and two clamps below the the T2 ganglion bilaterally. Postop pain the following day he described was significant when raising his arms but gradually diminished over time. His hands had become warm and dry immediately after that surgerybut he had only noticed a 40% decrease in his blushing and no improvement at all in his facial hyperpyrexia. He elected to have me perform Micro ETS of T2 todivide any missed Kuntz nerve branches present crossing the second rib and to divide the main sympathetic nerve by my micro cutting technique precisely at the upper border of the 2nd rib on each side. The patient underwent Micro ETS of T2 by me and I found a large Kuntz nerve 2mm under the pleural surface crossing the second rib approximately 2.5 cm lateral to the main sympathetic nerve trunk on the right side and 3.0 cm lateral to the main nerve on the left side. There were two metal clamps across the main sympathetic nerve at the second rib level and two at the third rib level (above and below the T2 ganglion). By my Micro
ETS technique, precise division of these Kuntz nerves was done
without having to remove a pleural window of tissue just to see
the nerves. After both sides had been precisely divided by my
Micro ETS technique, the patient's blushing completely resolved
as did his severe hyperpyrexia.
I find that the most common reason for recurrence of symptoms or failure to resolve them is missed Kuntz nerves crossing the second rib. The second most common reason for recurrence is mis-identified T2 where T3 is mistaken for T2 and the clamps or cutting is at the T3 level rather than the T2.
Please contact us for more information on hyperhidrosis: Call 210-490-7464 Email info@dhnmd.com or Submit a questionnaire.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

FACIAL SWEATING | SWEATY HANDS | SWEATY FEET | ARMPIT SWEATING | | ALTERNATIVE TREATMENT | IN THE NEWS
RESULTS MAY VARY FROM PERSON TO PERSON.
Copyright © 2021 Hyperhidrosis USA. All rights reserved.